A Quantitative Approach to Vaccine Funding
It is always easiest to insult your own work, so let me tell you what's wrong with the piece Rafael Dib and I just published on vaccine R&D.
Our analysis is driven by a practical question: how should Open Philanthropy spend money on science if we want to help as many people as possible? Our punchline is that R&D spending varies by 10X+ across diseases for no good reason. I've been poking at that punchline for the last six or so years, from different directions, and I am confident it's true.
But the heartburn in taking analytical approaches to practical questions is that any analysis faces tradeoffs between usefulness and accuracy. In this piece, we end up making all sorts of squidges in order to get to good-enough answers that are useful for our decision-making. When we don't have data for one disease, we make a best guess based on data from other diseases rather than leave a spreadsheet cell blank – we care about reality, not statistics. When we do have data, and subjectively think it's not "right" because it excluded some spending we would have included, or experts we've talked to think it's fishy, we don't follow the data source blindly. We're happy tweaking, but we can't rigorously defend those tweaks in a way all readers would agree with. (If you think we've gotten something important wrong, please email me or Rafa; we'd be very grateful!)
So that's why the academics reading the post should be mad at us: rigour was sacrificed for practicality. Here's why the practitioners should be mad: we sacrificed some important parts of the bigger picture story for the sake of a coherent piece. We scoped ourselves to vaccine R&D for this piece, which then gave us a defined list of infectious diseases. But, of course, there are many other health technologies worthy of similar R&D spending analysis – diagnostics, monoclonal antibodies, small molecule drugs, insecticides against mosquitoes, devices, gene therapies, hormones...
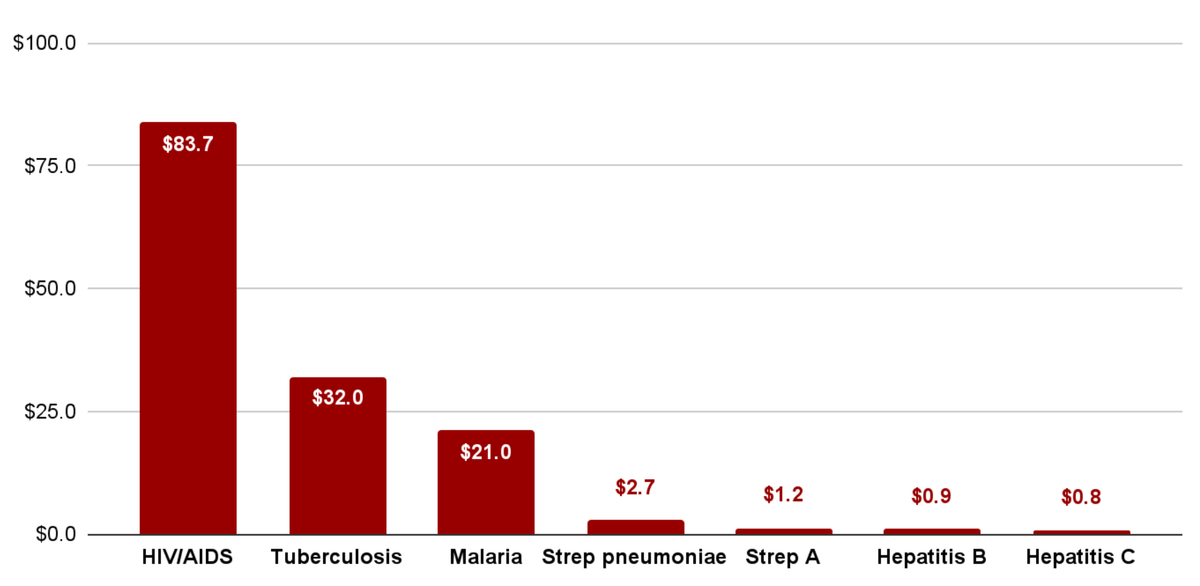
Our punchline that R&D spending varies by 10X+ across diseases for no good reason is actually missing some of the biggest variation, since we scoped ourselves down. Infectious diseases as a category receive vastly less R&D spending from industry than non-communicable diseases, per death they cause, because they disproportionately kill people in lower- and middle-income countries where the payoff for making a cure is less lucrative. In the image at the top of this post, TB and malaria look relatively well catered for. Yet cancer R&D spending is roughly $100 per projected 2050 DALY, to TB's $30, to strep A's $2. And there should be more cancer research spending, in my view, not less – just imagine how I feel about strep A!
So, my conclusion on our conclusion is that I believe it to be correct, but that there are more woods around these trees. What follows are sections 1 and 2 of the piece itself. Enjoy:
Introduction
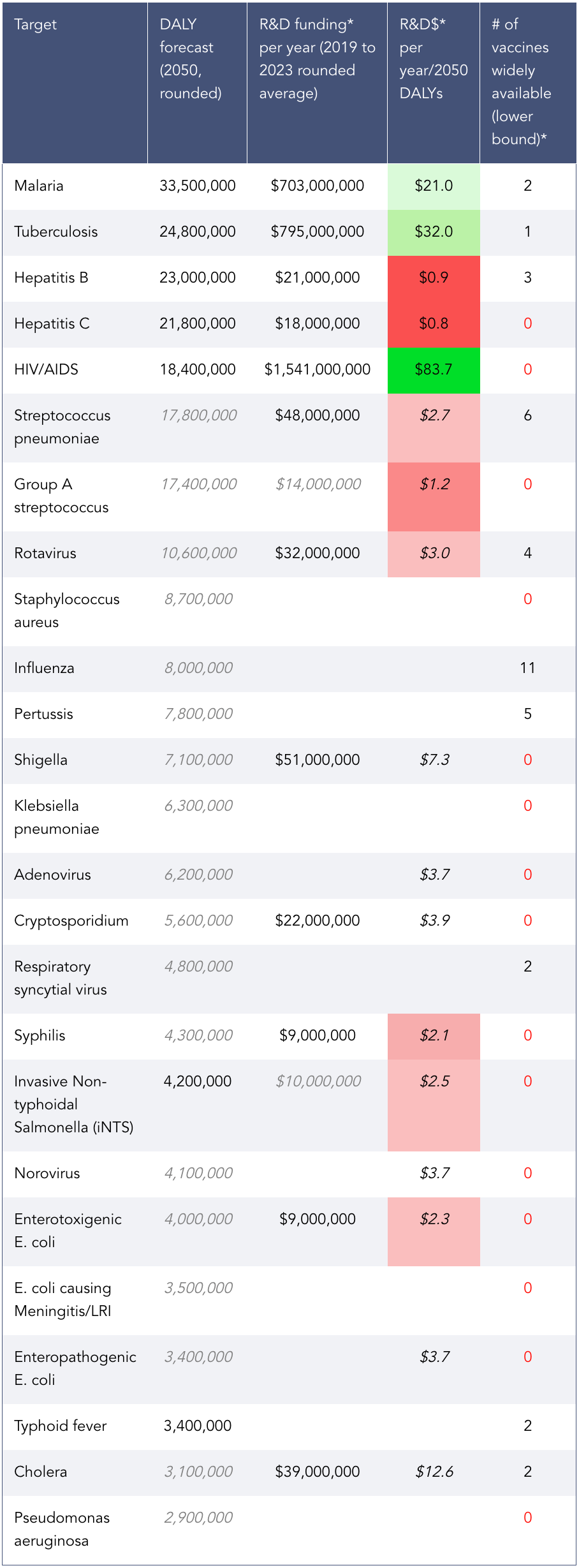
At Open Philanthropy, we often use the Importance, Neglectedness, and Tractability framework when making decisions about how to prioritise spending across cause areas. In this post, we apply the framework to vaccine research and development (R&D) by comparing potential vaccine targets using metrics of importance and neglectedness.
Our main takeaway from this exercise: some diseases that kill many people receive very few resources for developing cures and vaccines. In relative terms, R&D funding varies by 10 times or more across infectious diseases, often without good reason. This disparity suggests that science funders could find unusually high-impact opportunities by targeting the most neglected diseases.
We use importance-neglectedness analysis like this as a starting point for more specific scientific landscapes and grant investigations focused on tractability. Taken together, these analyses have led us to believe the development of group A streptococcus (strep A) vaccines, syphilis vaccines, and hepatitis C vaccines are promising areas for philanthropic support. (There are other areas of vaccine development we believe are also high impact, but for reasons that originate less in field-level neglectedness, and are more to do with importance and tractability.)
Past work on vaccine R&D
Since 2016, around 30% (or more than $150 million) of our grantmaking in scientific research and global health R&D has been related to vaccine R&D (inclusive of clinical trials).
We have made five or more grants for vaccine development in:
- Malaria
- Tuberculosis in adults and adolescents
- Strep A and rheumatic heart disease
- Syphilis
- Cross-cutting vaccine tools (computational models, animal models, new clinical protocols, new adjuvants, etc.)
We have also made grants in other areas of vaccine research when an opportunity seemed particularly strong. Sample areas include influenza, cholera, hepatitis E, schistosomiasis, and cancers (prophylactic).
Importance and neglectedness metrics
To read the rest of this post, go to the Open Philanthropy blog. The footnotes were finicky to reformat here.